

Introduction
This section gives guidance on how to use insulin safely and provides links to appropriate guidelines.

Who needs Insulin therapy
Type 1 diabetes (T1DM) is characterised by complete lack of endogenous insulin and treatment with insulin is the mainstay of therapy. In a newly diagnosed patient with Type 1 diabetes, insulin needs to be started as soon as possible. Insulin should never be stopped in a patient with Type 1 diabetes.
Type 2 diabetes (T2DM) is characterised by insulin resistance and progressive beta cell failure. High blood glucose levels can usually be controlled with non-insulin therapies (diet, oral and injectable treatments) for a period following diagnosis. However around 50% will require treatment with insulin within 6 years of diagnosis due to progressive decline of beta cell function.
In Type 2 diabetes, insulin therapy is initiated if individualised glycaemic targets are not met using diet and non-insulin therapies, if the individual is symptomatic e.g. rapid weight loss, polyuria, nocturia, if the individual has gestational diabetes (these women need to be managed in specialist care), in steroid induced diabetes (see “special circumstances ” section), if the patient is post myocardial infarction, if the individual is intolerant to non- insulin therapies, if the individual has acute neuropathies such as femoral amytrophy.
Initiation of Insulin therapy can be done in the community or hospital setting but it needs to be initiated by an appropriately trained and competent health care professional.
The UHL/LDC Insulin Therapies: An Educational Toolkit gives a good introduction for HCPs on elements of insulin initiation and management. Note: this document is written for the outpatient setting.
The table below shows the commonly used insulins and their profiles. Understanding how different insulins work is key to the safe use of insulin.
Inpatients on insulin therapy
The prevalence of diabetes among inpatients is increasing. The National Diabetes Inpatient Audit (NaDia) in 2017 showed that up to 17.5% of inpatients have diabetes of whom ~ 35 % are on insulin therapy.
For the majority (> 90%) of these admissions diabetes is a secondary diagnosis and not the primary reason for admission. These patients are often cared for by non-diabetes specialty teams.
NaDia highlighted key concerns in inpatient diabetes care. This audit showed that 18.6% of patients treated with insulin experienced an insulin error. Insulin is a high risk drug and if incorrectly prescribed, prepared or administered can lead to severe harm or death.
All the trainees should comply with insulin prescribing standards to minimise error.
Standards for Insulin prescribing:
Correct Brand name – beware of sound alike insulins (NB Humalog v Humalog mix25)
Correct device
Correct dose (check with pt, GP, etc.)
NEVER abbreviate “units” to “u” or “iu” due to risk of 10x overdose
Correct time
Correctly write on both charts (drug/EPMA and green chart)
Correct strength (U100, U200, U300, U500) eg, “(strength 200units/ml)”
The principles of a safe Insulin prescription can be summarized using the 6 R’s (graphic below)
Right person
Right insulin (brand)
Right strength
Right dose
Right time
Right device
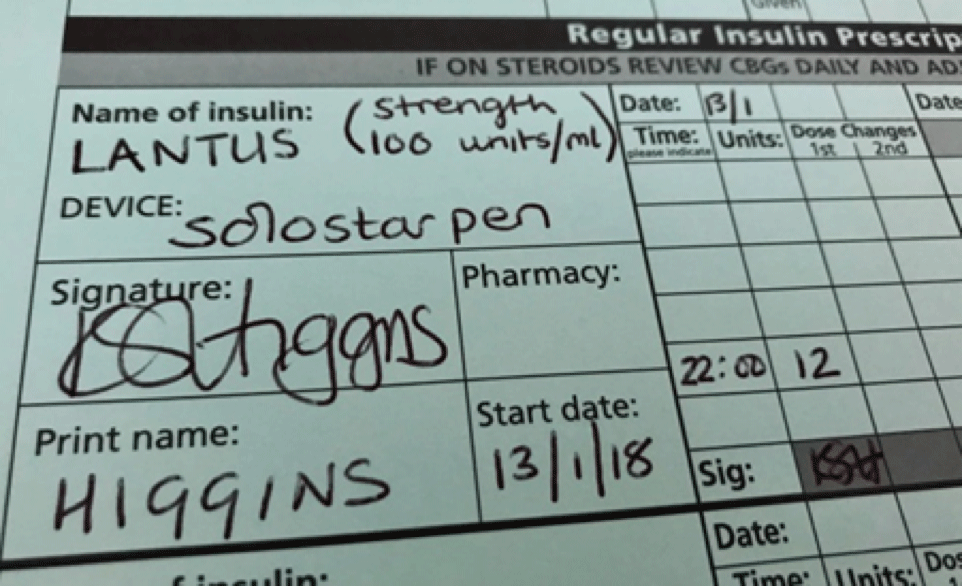
Below is an example of a safe prescription which meets the standards for safe insulin prescribing
Insulin preparation and administration
If you need to draw insulin up from a vial or administer insulin using a syringe and needle then this can only ever be done using a standard insulin syringes: 1ml syringes – for standard strength insulin (U100) 0.01ml = 1 unit insulin and 1ml = 100 units insulin.
If an incorrect syringe and needle are used there is a significant risk of insulin overdose and death.
NEVER use a syringe to withdraw insulin from an insulin pen cartridge. Pen cartrideges can only be used to administer insulin using an insulin pen.
Insulin is a time critical drug: Failure to administer insulin at the correct time may result in poor diabetes control or hypoglycaemia. Patients should have their insulin administered at the correct time which usually relates to their meal-times.